C1 esterase inhibitor deficiency

Leads to hereditary angioedema. Patients with this condition cannot be given ACE inhibitors.
C3 deficiency
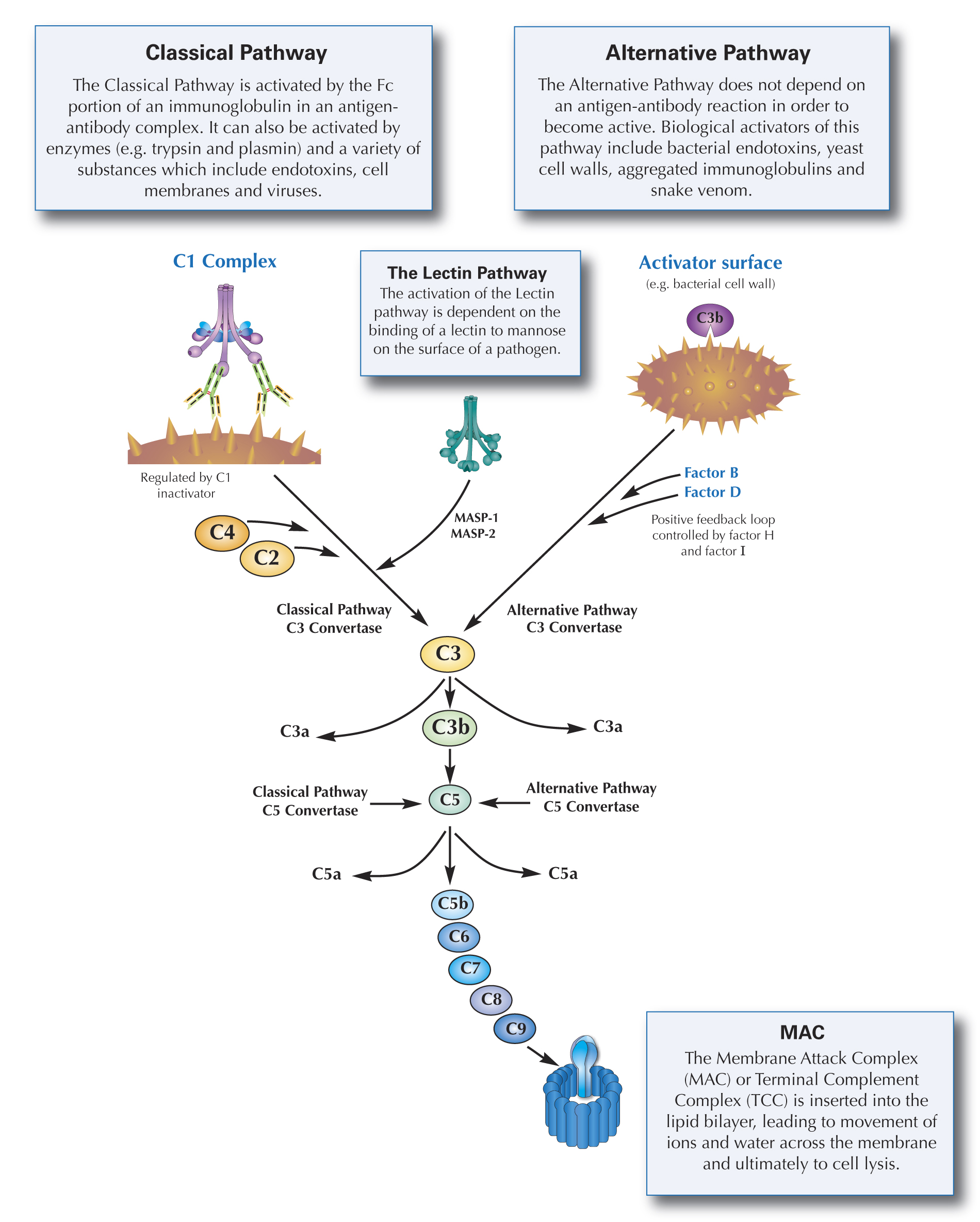
Leads to pyogenic sinus and respiratory infections with a high susceptibility to type III hypersensitivity reactions.
C5-C9 deficiency
Recurrent Neisseria infections.
DAF (GPI anchored enzyme) deficiency
Leads to compliment-mediated lysis of RBS and paroxysmal nocturnal hemoglobinuria (PNH).
Type I hypersensitivity
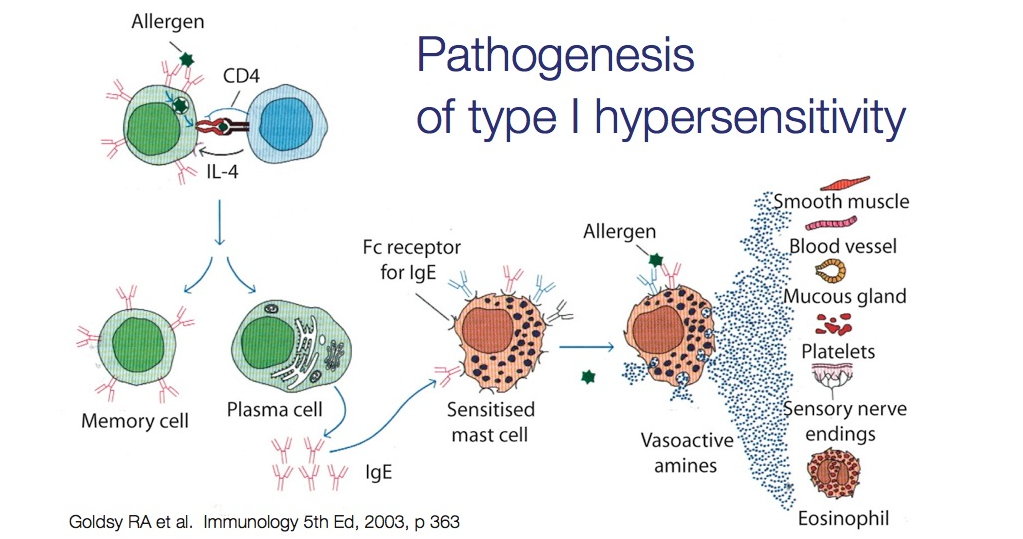
Rapid reaction to antigen due to preformed antibody. Massive release of histamine due to antigen crosslinking to IgE on mast cells and basophils.
Anaphylaxis (bee stings, food/drug allergies), hay fever, asthma.
This is immediate and can be seen on the skin.
Anaphylaxis (bee stings, food/drug allergies), hay fever, asthma.
This is immediate and can be seen on the skin.
Type II hypersensitivity
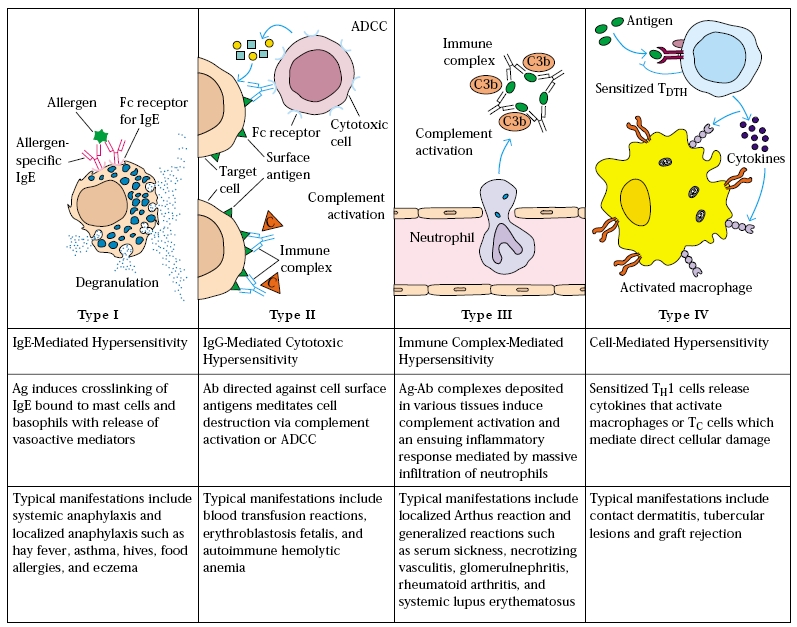
"Cytotoxic" - antibody mediated leading to formation of MAC. IgM and IgG bind to antigen and trigger opsonization, lysis, or ADCC utilizing NK cells.
Autoimmune hemolytic anemia, pernicious anemia, idiopathic thrombocytopenic purpura, erythroblastosis fetalis, rheumatic fever.
Disease will be at tissue site.
Autoimmune hemolytic anemia, pernicious anemia, idiopathic thrombocytopenic purpura, erythroblastosis fetalis, rheumatic fever.
Disease will be at tissue site.
Type III hypersensitivity
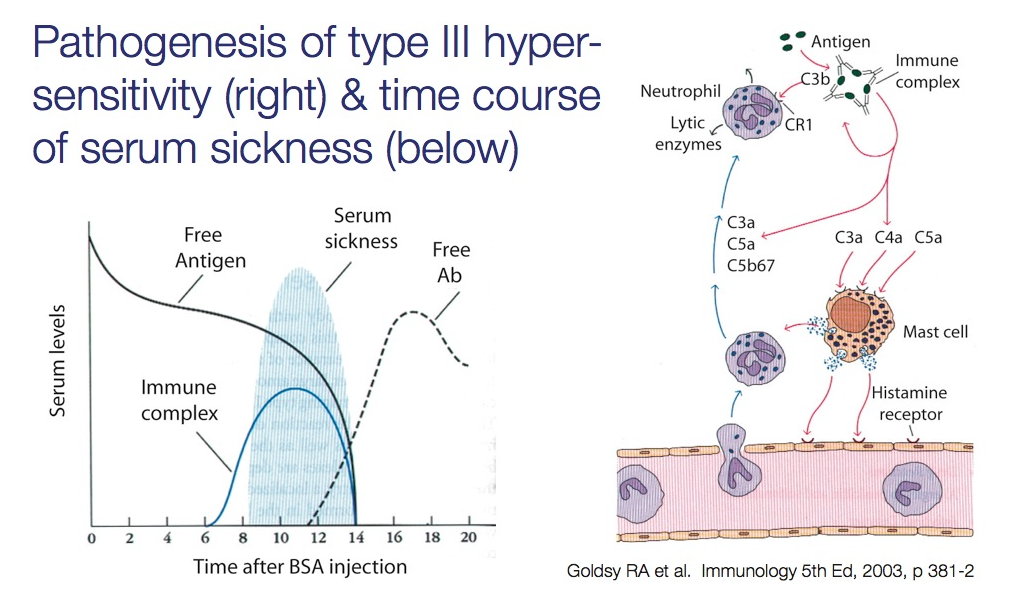
When antibody-antigen-complement complexes form leading to tissue damage. Utilizes IgG and neutrophils releasing lysosomal enzymes.
Serum sickness is a type III often caused by drugs.
Arthus reaction is a type III which occurs with intradermal injections of antigen followed by edema, necrosis, and complement.
SLE, poststreptococcal glomerulonephritis, serum sickness, and arthus reaction.
Vasculitis seen as well as systemic manifestations.
Serum sickness is a type III often caused by drugs.
Arthus reaction is a type III which occurs with intradermal injections of antigen followed by edema, necrosis, and complement.
SLE, poststreptococcal glomerulonephritis, serum sickness, and arthus reaction.
Vasculitis seen as well as systemic manifestations.
Type IV hypersensitivity
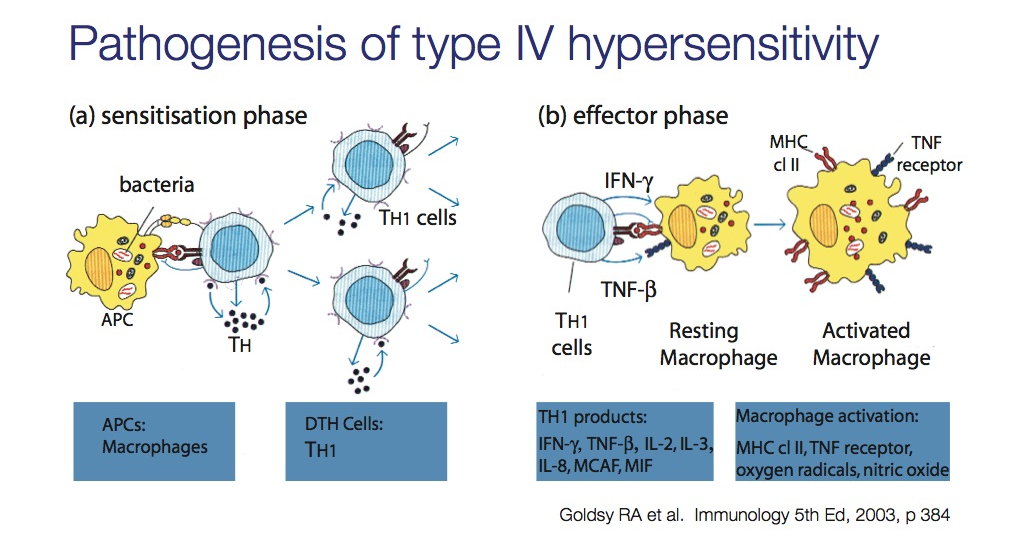
This is the delayed type of which T cells activating macrophages is responsible. This occurs in transplant rejection and TB skin tests.
Multiple sclerosis, Guillain-Barre syndrome, Graft-versus-host, PPD for M. tuberculosis, contact dermatitis (poison ivy, nickel allergy).
Delayed response without antibodies.
Multiple sclerosis, Guillain-Barre syndrome, Graft-versus-host, PPD for M. tuberculosis, contact dermatitis (poison ivy, nickel allergy).
Delayed response without antibodies.
Blood Transfusion Reactions (the following 4)
Allergic
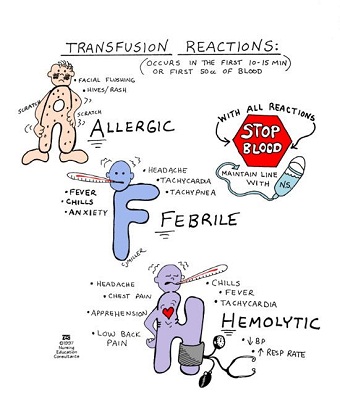
Urticaria, pruritus, wheezing, fever... all due to a type I against plasma proteins in transfused blood.
Anaphylactic
Dyspnea, bronchospasm, hypotension, respiratory arrest, shock... all severe... happens when IgA deficient patient does not receive IgA deficient blood.
Febrile nonhemolytic transfusion reaction
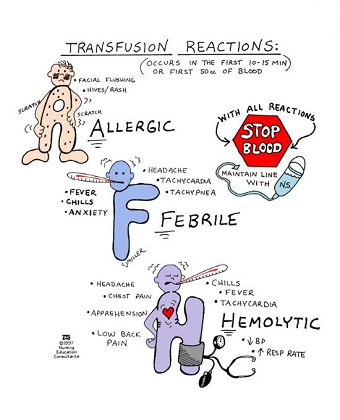
Fever, headaches, chills and flushing due to a type II from host antibodies attacking donor HLA and leukocytes.
Acute hemolytic transfusion reaction
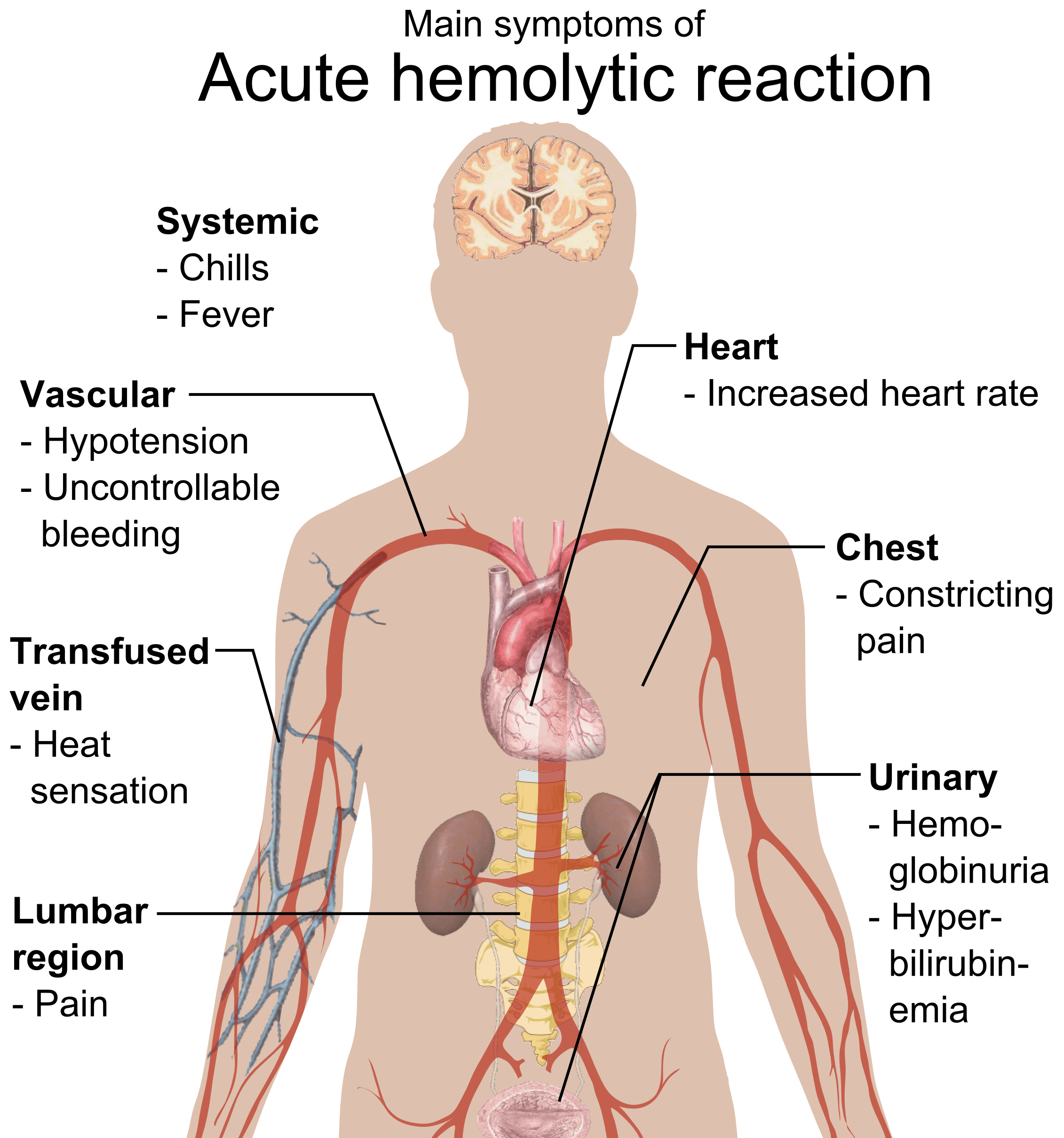
Fever, low BP, tachypnea, tachycardia, flank pain, hemoglobinemia, jaundice from a type II reaction. ABO mismatch resulting in hemolysis.
X-linked (Brutons) agammaglobulinemia
You'll find that the infant will get recurrent bacterial infections as of 6 months of age. There is a loss of maternal IgG and the opsonizing effect. It is XR at the BTK gene (a tyrosine kinase) leading to no B cell maturation. There will be a decline in all classes of Igs.
Selective IgA deficiency
The most common primary immunodeficiency and we don't know what is defected. There is low IgA. The majority of patients present asymptomatically but may get sinopulmonary infections, GI infections, and will have an anaphylaxis reaction to donated blood which contains IgA.
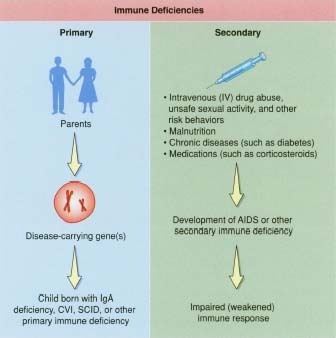
Common variable immunodeficiency (CVID)
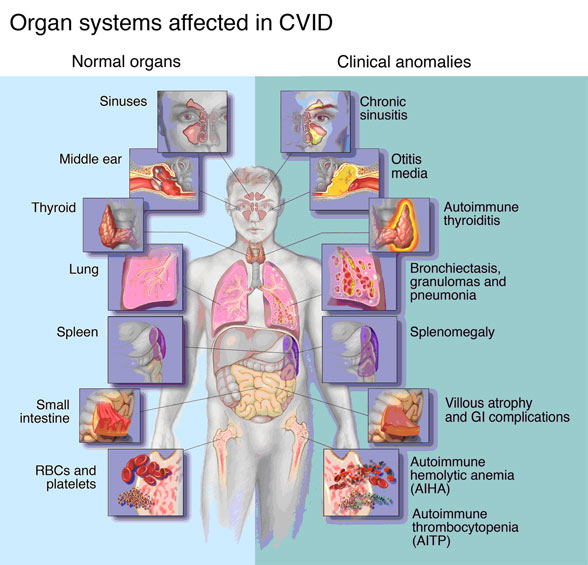
This may happen in 20s and 30s increasing risk of autoimmune disease, lymphoma, and sinopulmonary infections. What happens is that there is a defect in B-cell maturation resulting in low titers of plasma cells and Ig.
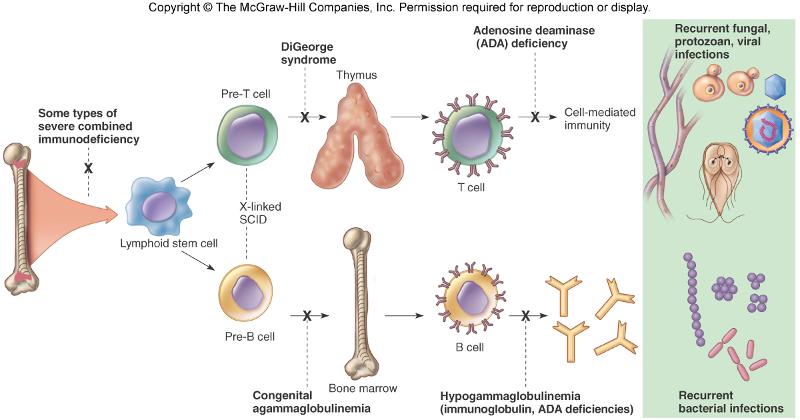
Thymic aplasia (DiGeorge syndrome)

Thymus and parathyroids fail to develop resulting in low T cell levels and low PTH, and thus, low Ca. If you take an X-ray, there will be an absent thymic shadow. It's from a 22q11 deletion and the failure of the 3rd and 4th pharyngeal pouches to develop. Patient will constantly get viral and fungal infections, have congenital heart disease and many vessel defects.
with autism: http://www.youtube.com/watch?v=Q8RpR9S22_8
with autism: http://www.youtube.com/watch?v=Q8RpR9S22_8
IL-12 receptor deficiency
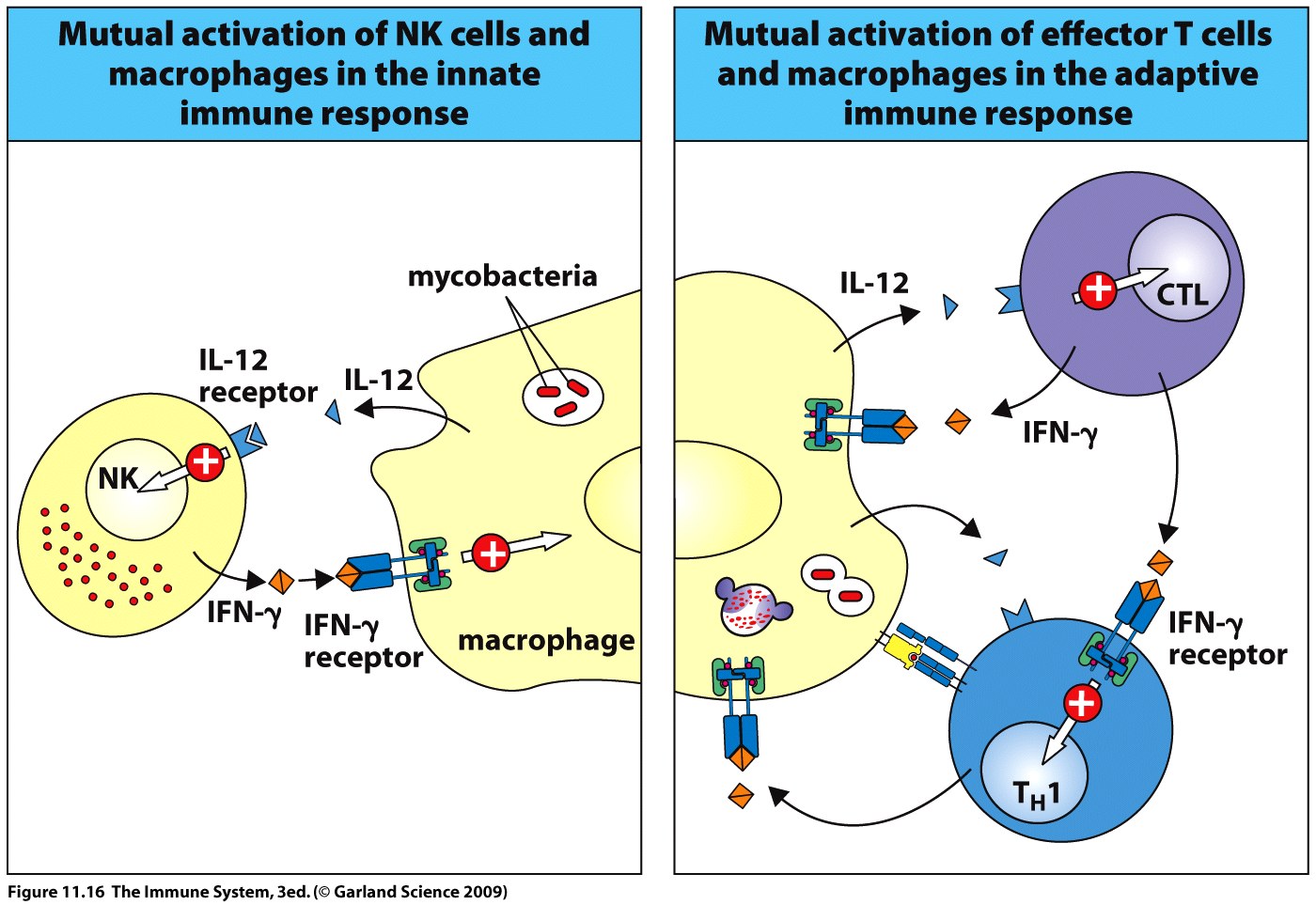
Th1 cannot respond and so, IFN-gamma levels will not increase. Patient will get a lot of mycobacterial infections.
Hyper-IgE syndrome (Jobs syndrome)

You can tell a patient has this by using the acronym FATED: coarse face, staphylococcal abscesses, retained primary teeth, high levels of IgE, and dermatologic problems. The Th1 cells fail to produce IFN-gamma and so, neutrophils cannot respond to chemotactic stimuli.
Chronic mucocutaneous candidiasis

T cell dysfunction leading to Candida albicans infection on the skin and mucous membranes.
Severe combined immunodeficiency (SCID)

Low or no T cells, absence of thymic shadow. Can be from several things but an X-linked defective IL-2 receptor is the most common. Can also be due to adenosine deaminase deficiency.
There is failure to thrive, diarrhea, recurrent infections. Only treatment is a bone marrow transplant.
There is failure to thrive, diarrhea, recurrent infections. Only treatment is a bone marrow transplant.
Ataxia-telangiectasia

Defect in ATM gene which codes for DNA repair enzymes. High levels of AFP. Presents with a triad: cerebellar defect (ataxia), spider angiomas (telangiectasia, & IgA deficiency.
documentary: http://www.youtube.com/watch?v=a_h8aOg0F5E
documentary: http://www.youtube.com/watch?v=a_h8aOg0F5E
Hyper-IgM syndrome
High IgM but low G, A, & E. Leads to pyogenic infections early in life. It is the CD40L on helper T which are defective and so, class switching is not possible.
Wiskott-Aldrich syndrome
High IgE and IgA but low IgM & thrombocytopenia. The triad is TIE: thrombocytopenic purpura, infections, eczema.
WAS gene of the X chromosome. T cells become unable to reorganize their actin cytoskeleton.
WAS gene of the X chromosome. T cells become unable to reorganize their actin cytoskeleton.
Leukocyte adhesion deficiency (type 1)
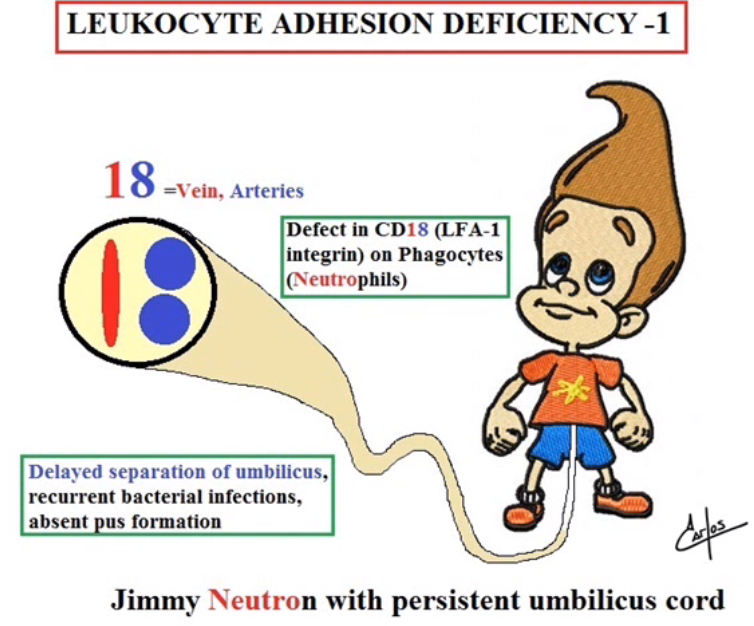
Neutrophilia due to a defect in the LFA-1 integrin (CD18) protein on phagocytes. Patient will get bacterial infections and there will be a delay in the separation of the umbilical cord.
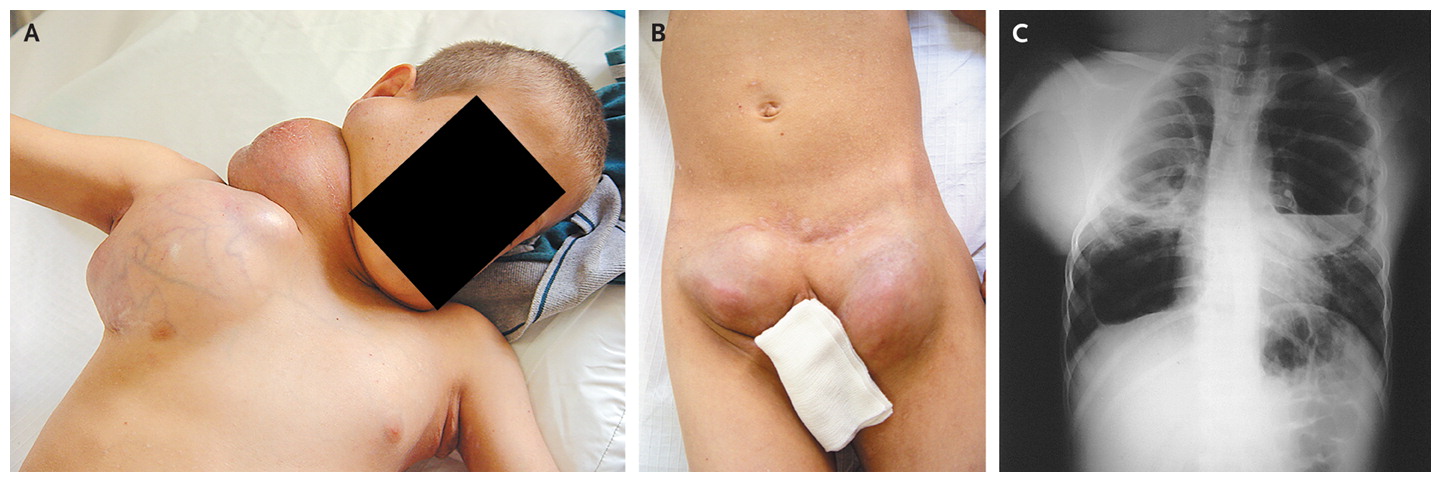
Chediak-Higashi syndrome

Giant granules in neutrophils from an AR defect in lysosomal trafficking regulator gene (LYST). There is a microtubule dysfunction in phagosome lysosome fusion. Patient gets pyogenic infections and staphylococci as well as streptococci, partial albinism, and peripheral neuropathy.
Chronic granulomatous disease
Lack of NADPH oxidase leads to low levels of ROS and therefor, a poor oxidative burst. So, you get a lot of catalase positive organism infections like: S. aureus, E. coli, and Aspergillus. Findings will show an abnormal dihydrorhodamine (DHR) flow cytometry test. A nitro blue dye reduction test is no longer used.
